This fact box can help you to weigh the benefits and harms of a routine incision of the perineum (episiotomy) during vaginal birth. The information and numbers are based on the best scientific evidence currently available.
This fact box was developed by the Harding Center for Risk Literacy.
The perineum is the area between the vagina and the anus. During vaginal birth, this tissue stretches significantly in order to allow the baby’s head to pass through the vaginal opening. This can cause tears to the vagina and the surrounding tissue. In some cases, the tissue tears all the way to the anus [1].
An episiotomy is an incision of this tissue, which is under a lot of pressure during labour, towards the anus. It is meant to enlarge the vaginal opening in a controlled way, so as to prevent severe injuries (e.g. deep tears of the tissue) to the mother or to reduce the risk (e.g. of poor circulation or breathing Problems) for the baby. A further reason why an episiotomy might be necessary is, for example, a breech birth [1].
In general, the episiotomy is carried out during the second stage of labor. If it has not already been administered, a local anesthetic is injected before the cut. Like a perineal tear, the incision is stitched up after the birth [1].
Episiotomy is one of the most common surgical procedures worldwide. In some countries, it is part of standard care during childbirth, whereas in others it is only carried out if necessary [1].
When a vaginal birth entails potential complications or is unwanted, a caesarean section (C-section) can be performed instead. During a caesarean section, the abdominal wall and uterus are opened to remove the baby. The operation is performed under either full or partial anesthesia and takes about an hour. Afterwards, the uterus and the abdominal wall are closed with sutures [2].
According to the World Health Organisation (WHO), a caesarean section is necessary in around ten to 15 percent of births in Western countries.
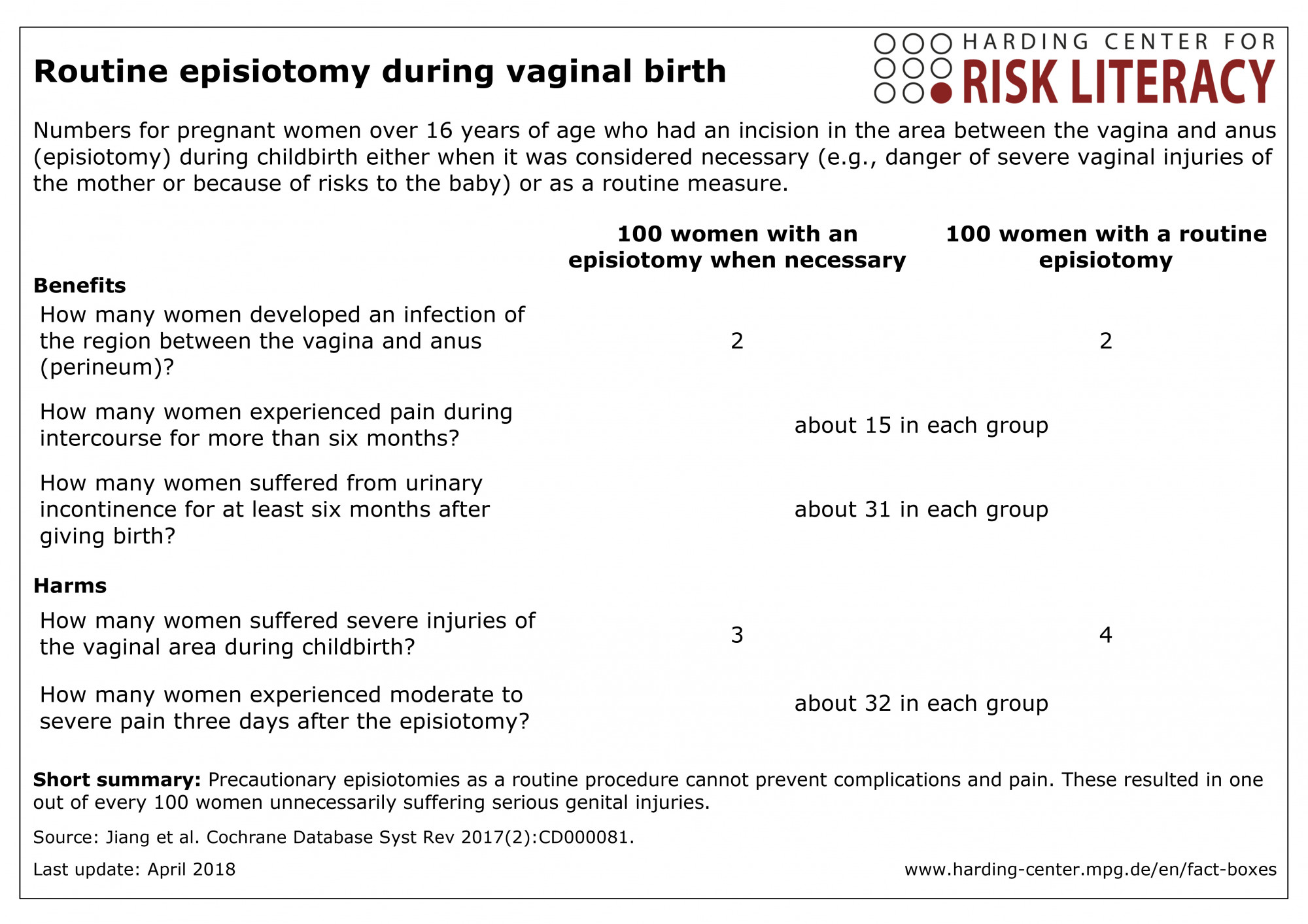
The fact box shows the benefits and harms of an episiotomy when it was necessary compared to one carried out as a routine measure.
The table may be read as follows:
Approximately 2 out of every 100 women who had an episiotomy either as part of standard treatment or out of necessity developed an infection of the perineum.
The numbers in the fact box are rounded. The data were reported in twelve studies with 6,177 participants [1].
Pain was not carefully assessed in any of the studies used in the review. Women were also not asked about their preferences regarding the birth.
Further important outcomes in terms of long-term effects of prolonged, complicated labor, such as an abnormal connection between the bladder and vagina (vesicovaginal fistula) or between the vagina and anus (anal fistula), which can occur due to pressure sores or stool incontinence were not reported in the studies.
Overall, the evidence is of low to moderate quality:
Further research is very likely to affect the findings regarding severe injuries, perineal infections, urinary incontinence for more than six months, and pain three days after the episiotomy (low quality of evidence).
Further research is also likely to affect the findings regarding pain during intercourse for longer than six months (moderate quality of evidence).
- April 2018 (development)
Information within the fact box was obtained from the following sources:
[1] Jiang H, Qian X, Carroli G, Garner P. Selective versus routine use of episiotomy for vaginal birth. Cochrane Database Syst Rev 2017(2):CD000081.
[2] Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen (IQWiG). Kaiserschnitt 2018 [Available from: https://www.gesundheitsinformation.de/kaiserschnitt-welche-vor-und-nachteile-haben.2686.de.html accessed 27.03.2018]